
The High-Functioning Depressive
My personal two-and-a-half year battle with Major Depressive Disorder

In 2017, I was speeding down I-95 at 80 mph from my home in NYC to my office in Rahway, New Jersey, and I wondered how often car accidents are due to suicide. I had been dealing with a long period where nothing could make me happy, and where I wasn’t even sure I could ever feel that way again. I remember seeing a mom and her child in a playground sharing a laugh through the window of a restaurant. While I had such experiences myself in the past and understood their joy on an intellectual level, emotionally, I couldn’t imagine simple happiness right then and wasn’t sure I would ever have it again.
My depression had started because of workplace trauma. I had been under tremendous pressure for three years working on the approval of sugammadex (Bridion) at Merck Research Laboratories. After a setback earlier that year, when my trial was accused by an inspector of possibly including malfeasance, we successfully challenged the FDA, which accepted the trial’s integrity in June 2015, after which we submitted the New Drug Application to the FDA almost immediately. After an Advisory Committee Meeting in November 2015, which issued a unanimous recommendation for approval, the FDA finally approved our application on December 15, 2015. I should have been overjoyed, but instead, I felt numb inside. I felt like the rejection, or Complete Response Letter, from the FDA in April 2015 was my fault. Given that this is now more than a $ 1B-a-year drug in terms of revenue, you could say I cost the company $750 million in revenue.
Even though the company’s management didn’t blame me for my debacle, as I surely would have been fired if they had, I couldn’t help but blame myself. As word of the approval spread, accolades showed up by email, text message, and Jabber (does anyone miss that messaging system from Cisco?), and I simply rolled my eyes and shrugged. Three friends from work took me out for a celebratory dinner at the Harvard Club in New York. We had a lovely evening, but I could only feign enthusiasm. I tried my best to go through the motions, but I felt no joy. The same applied to my enjoyment of a family vacation to Sea Island, Georgia, that Christmas. I knew I had to do something about my depression, so I told Amy that I would go see a psychiatrist.
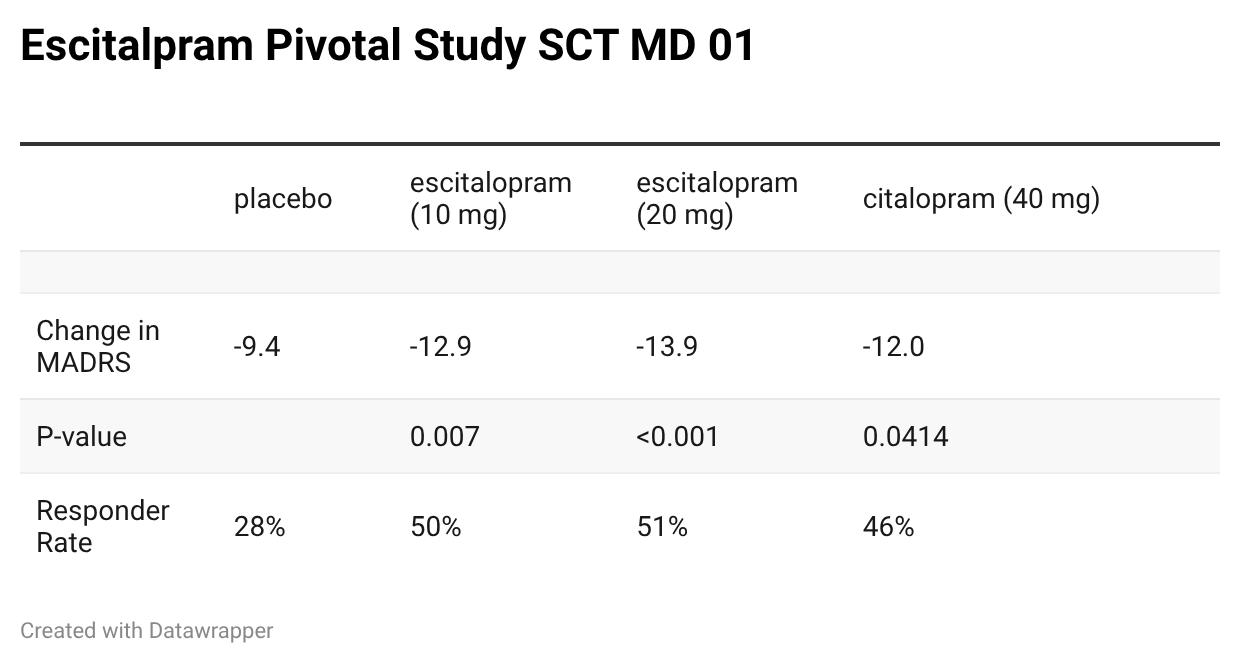
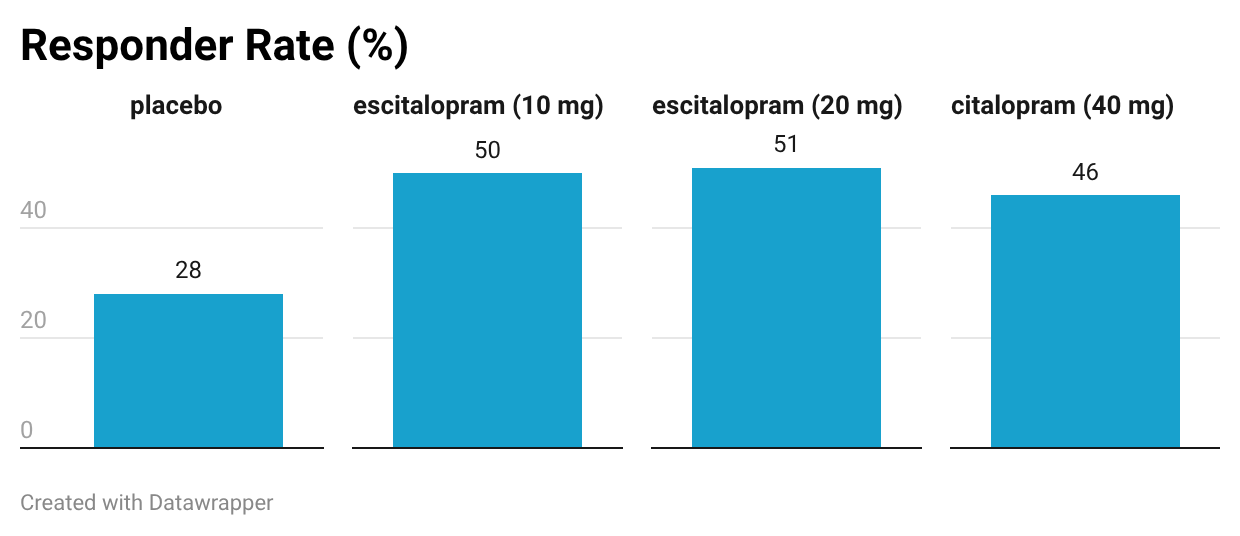
That psychiatrist prescribed an SSRI (selective serotonin reuptake inhibitor) to help treat my depression. I started with Prozac, and when that didn’t appear to help after four weeks, we switched to escitalopram (Lexapro). In my case, my psychiatrist tried a higher-than-normal dose of 30 mg of Lexapro because my depression was so resistant. Because I complained of low energy and poor concentration, we also tried stimulants used in the treatment of ADHD (attention-deficit hyperactivity disorder) as well.
To this day, I am not sure whether any of these medications helped. I guess that they may have helped somewhat. In clinical trials, about half of the patients had a dramatic response (a lowering of their depression score by 50% or more), whereas the other half of the patients had a less dramatic response. I feel like I was in that half with a less robust response to treatment with SSRIs.
In addition to receiving Lexapro from a psychiatrist, I worked with a behavioral psychologist. She was wonderfully supportive, but I found my therapy ineffective. For nearly a year, I saw her every week. Things didn’t get better. Part of the problem was that I knew so much about my disease—after all, as a neurologist, I had treated many patients for depression. I knew that Cognitive Behavioral Therapy could be effective, and that the “fake it until you make it” approach actually works for many people. Nothing seemed to work for me. After about one year, I stopped taking antidepressants and quit psychotherapy. I was having various side effects from the medication, and I suspected it wouldn’t make much of a difference in my mood if I quit, so I gently tapered them to nothing. I didn’t notice a significant difference in my mood.
From December 2015 until June 2018, I went through the motions; I exercised by taking spin classes at Soul Cycle with Amy, played in my chamber orchestra, and participated as much as I could in family activities. Throughout that period, I was still able to function at work. I never missed a day and delivered my assignments on time. My performance reviews, while not stellar, had me in the broad category of “meeting expectations.” Given the intense environment at MRL and the fact that my level of Clinical Directors was under intense pressure to perform, I would call the expected “average performance” a little above normal, like how Garrison Keillor describes the children of Lake Woebegone on his long-running Prairie Home Companion Program as all being “above average.[NK1] ”
While I did receive satisfactory reviews, my performance at work had deteriorated. I realized I needed to get engaged in a challenging project. I tried to volunteer for interesting assignments at Merck, but those efforts were unsuccessful. For example, there was an interesting program to develop a novel antibacterial therapy. This would require me to learn a completely different medical area, infectious disease. far afield from neurology. Moreover, since our cross-functional personnel tended to specialize in therapeutic areas, I would have to interact with an entirely new set of colleagues. I got excited about the prospect of taking on such a challenge, but then became overwhelmed as I started meeting my various team members. I had been open with my management about my struggle with my mental health before taking on this project, so thankfully, they understood when I ultimately chose to withdraw from leading that program. Perhaps if I had stuck with it, I might have pulled through, but work was the source of the original trauma for me. In the end, I just couldn’t stomach putting everything necessary into the project.
Being depressed puts you in a strange existential state. I intellectualized it, thinking I simply “needed to get better,” and I would even beat myself up about it. During this time of my life, I was a terrible partner to Amy and wasn’t present as a father to my girls. I did all sorts of nonproductive things. A typical example was starting a 13-part Marvel series on Netflix at 11 pm before going to bed. I wasn’t interested in the storyline, and thought the writing and acting were awful. But it temporarily took my mind off other things—what those things were, I honestly couldn’t say. I just wanted to escape them. In addition to bingeing on Netflix all night, I worked through the entire archive of the New York Times crossword right back to the very first one on Sunday, February 15, 1942. I don’t believe the current version of the app lets you go back that far, but I completed every crossword (yes, sometimes cheating with hints). I also got into the habit of playing Madden Football on my iPhone. It was a stupid pursuit, especially given the crude controls. I remember one of my daughters, Libby, would roll her eyes as I ignored the family conversation at dinner while playing the game.
Not surprisingly, given my poor sleep habits, I was involved in many car accidents during my 1-hour commutes in both directions between Rahway, New Jersey, and my home in Manhattan. During the two-and-a-half years of my depression, I got into six single-car accidents and was dropped by every insurer in the state of New York. I found out the hard way that there is a state-run insurer of last resort for people like me. It was called Integon, and given their clientele, they do not compete on niceties like customer service. For a while, we paid over $24,000 per year for auto insurance so I could drive my eight-year-old Honda Odyssey back and forth to work.
I had many near misses in addition to those six accidents. Sometimes during my commute, I would stream those stupid Netflix series on my phone while driving. Doesn’t that make that character, Mayhem, in Allstate Insurance commercials seem like an amateur? I became fascinated by the concept of suicide by car accident. I found myself wondering how often people commit suicide by auto accident, and I Googled the topic during that time. What I found out through various websites was that there are quite a few accidents suspected of being from a suicide attempt, but that they are not classified as suicide unless there is specific evidence, such as a note left saying that was their intent.
As a society, we have made great progress in recognizing mental health issues compared to decades past, but there are persistent deficiencies, especially for professions like medicine. For example, I find it reprehensible that, as a physician, on the first page of forms for malpractice insurance at a hospital, one often has to answer the question, “Have you ever had a mental illness?” This is placed just after the question about whether you have ever been convicted of a crime. Despite criticism by various professional societies such as the AMA, this practice continues. It is particularly galling since the lifetime prevalence is about one-fifth of the general population; furthermore, physicians are among the professions least likely to seek help. One example is Dr. Lorna Breen, an emergency room physician and head of the Emergency Department at the Allen Pavilion at New York-Presbyterian Hospital in Manhattan. Worried she would lose her medical license and damage her reputation while suffering greatly during the stress of the COVID-19 frontline response, she committed suicide in April 2020. Because licensing boards across the country require that physicians disclose any mental health care, her father blamed her work for her reluctance to get the support she needed, which ultimately led to her death.
One of those was a friend whom I’ll call TDA. Recently promoted to Clinical Director, TDA felt pressure to prove himself, especially given that he didn’t have the advanced degrees of most of his colleagues. This is the typical plight of overachievers—a desperate need to prove oneself, when in fact, one has already been proven. TDA took on his new role with gusto, along with his first challenging assignment: chairing an Early Development Team (EDT). EDTs are composed of a multidisciplinary group of about eight scientists, including a medicinal chemist, a biologist, a toxicologist, a clinical supplies expert, a statistician, a pharmacokineticist, and a clinical scientist. Everyone reports to their respective functional area heads. While every member does try to contribute to the team’s objectives, they also play a role in fulfilling their departmental objectives, which can sometimes conflict with the team’s goals. TDA needed to navigate through those conflicts while developing a strategy and timeline, which is then often criticized by management for perceived gaps in opportunities to accelerate development. The chair often juggles team priorities while constrained by budgetary allowances and resources allocated to ~20 other EDTs. Chairing a single EDT is a challenging job.
TDA took on the chair role for two different EDTs, which is usually too much work for a single person. He convinced himself that he could manage it because one team was in a relatively quiet mode. However, as often happens, the second team became more active, and he was now straddling two teams, trying to run at full speed, like the trick rider in the video below. Everyone in the department knew about his predicament and thought that he had too much work. I remember sitting down with him and asking how things were going, and he explained how hard it was. I told him to give up one of his programs, but he insisted he could manage it. I later found out that when he shared his anxieties with his manager, she responded like a cheerleader, exhorting him with, “You can do it!” I don’t think his manager had bad intent; rather, she lacked awareness. Unfortunately, TDA was finally pushed past his breaking point. One day at work, he broke down, unable to do anything but curl himself into a ball and cry at his desk. He almost couldn’t drive himself home because he was in such a state. He belatedly sought help from a psychologist and was only able to come back to work after several months away on disability leave. Even then, he suffered from PTSD because of his experience.
The situation with TDA occurred during the buildup to my own depressive episode. I tell this story because it is so common in high-pressure workspaces where managers are woefully inadequate. MRL is a wonderful company that prides itself on developing strong leaders, as does every good company that has received the “blessing” of advice from management consulting firms. However, there is a massive blind spot in corporate America. The focus and drive toward productivity are about maximizing deliverables, not the holistic well-being of employees, not even those employees who are in management. While TDA and I were suffering, another member of the department took a disability leave for treatment of her anxiety. Three out of about twenty of us were disabled by the pressures of work combined with a psychiatric response. I also think we need to change our attitudes about mental illness in the workplace.
Let us consider how such situations are dealt with in corporate America. We have already noted that the prevalence of major depression is 8-9% of adults each year. Imagine if you also add anxiety disorders to that total. We have already discussed the inappropriate singling out of mental health for malpractice insurance by doctors—why don’t they ask about other health conditions that could lead to disability, like rheumatoid arthritis? When I saw my psychiatrist, he noted that my care was covered by my insurance plan but recommended I just pay the bill with a credit card. Why? Because he knew the consequences. Having insurance payments for my psychiatric care would then be on my permanent health record, resulting in potential problems for malpractice insurance applications and for hospital appointments. While we have come a long way towards recognizing psychiatric illness as a challenge in our society, it is still treated as a taboo subject. Given how impactful these diseases are, when was the last time you heard of management training to deal with mental health issues? [NK1]
Do you know anyone at work who took an unexplained leave of absence? When that person returned to work, did you ask how their recovery was going? Did others inquire, or did everyone just keep it hush-hush out of privacy concerns? Compare that to someone who goes out for an acute illness like pneumonia, or someone who needs elective surgery to get a hip replacement. No problem to discuss openly the good news that someone has recovered or is on their way to a better future, right? We all need to be better equipped for conversations concerning mental health if we want a healthy work environment. Perhaps more importantly, we need to be able to ask about things before someone needs to take a leave. Often, many of us can recognize when someone is struggling at work, yet how many of us have the empathy and courage to ask them about it? Yes, it could lead to deeply personal conversations, but your inquiry could even prevent a suicide.
Granted, we can’t expect to be trained by our workplaces to treat mental illness, and many of us would probably elect not to, even if such training were offered. What I am suggesting is that we could do much better as peers and managers in helping someone seek help when they need it. When someone is suffering from mental illness, it can be so overwhelming that they don’t know what to do. In my opinion, having explored the options available at MRL and assuming those options represent best corporate practices, our current workplace resources are not designed with the employee’s well-being foremost.
The manager’s main role appears to be identifying underperformers due to such challenges and referring them to HR immediately. I think that is the first misstep. Typically, an employee does not have a well-developed relationship with the HR representative. While the system is ostensibly designed to connect an employee with available corporate resources, there also seems to be a strong interest in ensuring the employer’s limited liability. As a CEO, I acknowledge these concerns, but I believe valuing employees means balancing the interests of the corporation and the well-being of employees in different ways. Managers should be trained to understand that such conditions are common, to evaluate their own behavior and consider changes they can make to avoid contributing to such problems before escalating, and to actively participate in connecting the employee to resources and to monitor the recovery process.
From December 2015 to June 2018, I kept trying to “fake it till I make it,” but went nowhere. I felt like a car in first gear trying to shift directly into fifth gear. There are many different types of people, from those who are always in first gear, like Eeyore in A. A. Milne’s Winnie the Pooh, to those who seem to live in fifth gear, like the excitable Tigger. Perhaps Pooh himself would be in third gear, neither super excited nor sad. Some cycle across the different gears, going from Tigger down to Eeyore, then back up to Tigger. At the time, I was the kind of person who just cruised in fifth gear; people would call me a positive person—until the major depression, I had no real experience in either depression or those lower gears. I knew I needed something to activate me, to somehow pop the clutch to go from 1st to 5th gear without stalling.
The project that saved me was buying a new home. One Sunday in June 2018, Amy’s sister, Alice, was visiting from London, and we went to an open house for a three-bedroom apartment in the same building in which we lived. At the time, our family of four lived in a two-bedroom apartment, with our teenage twin girls sharing a single bedroom with a bunk bed. When looking at the three-bedroom apartment with Alice, I remember thinking it was an odd open house. For me, a typical open house had the front door propped open, refreshments on the dining table, and a printout of the key parameters, including the floor plan. Various shoppers would wander through the apartment, looking at the rooms, while the realtor was on hand to answer any questions. That was not the case on that Sunday afternoon.
Alice and I had to dial a number to set a time to see the apartment. Since we lived in the building, we agreed to meet at the apartment door rather than down in the lobby. The realtor opened the door, and we saw an empty apartment with no refreshments, no decorations, just a slightly dusty interior with bare walls. The realtor commented that no one tends to show up for open houses these days, so she was doing the showings by appointment.
After we got back, Alice commented that she thought the apartment was overpriced. I was mildly offended. She is a Londoner, I thought, what the heck does she know? I decided to look at StreetEasy.com. This is kind of like a Zillow real estate platform that is specific to the city of New York. Shopping online for apartments is considered a bit of a bloodsport for New Yorkers. People spend many hours on the site, even if they aren’t remotely able to afford a new place, just to fantasize about possibilities. Whether they own or rent, no true New Yorker is completely satisfied with where they live—they’re always looking for something a bit more spacious, fancier, or with better amenities or views, or something that better reflects their perceived social standing.
In any case, over the more than 20 years that we lived in our generously sized two-bedroom apartment, I frequently looked on Street Easy for three-bedroom apartments. The search that day revealed a much larger inventory than I had routinely seen in the past. Furthermore, I noticed that much of the inventory was stale, with some homes on the market for more than a year, and that some homes were marked down by $100k or $200k from their original asking price.
I thought to myself, Maybe Alice is right, and we are in a buyer’s market! I first perused our various accounts and was surprised to discover that our cash position was better than I had realized. In addition to our normal bank accounts, we had squirreled away money in a few different high-interest-bearing accounts. The next thing I did was make some very crude estimates of monthly mortgage payments in an Excel spreadsheet, using different parameters, assuming the generally low interest rates available at the time, and varying the price for buying a new three-bedroom and for selling our current two-bedroom. I quickly realized that this was going to be a complicated process with a fair amount of risk. The challenge in New York is that one cannot buy a property on a contingency basis. Instead, you typically make a no-contingency offer and begin selling your home only after it is accepted. At a minimum, you will end up paying a mortgage on both properties for a few months. If you’re truly unlucky, you need to carry two mortgages for six months or more.
The complexity of this process was exactly the kind of challenging project I needed to activate my mind. Better yet, it forced me to rely on others for help. I reached out to one friend who had an amazing realtor, whom she thought helped her only because they were both parents of children at the same private school. I reached out to another friend, who told me that they had met a fantastic closing lawyer who, unfortunately, worked for the other side in a transaction. I contacted my mortgage banker, whom I had befriended in our last purchase. Then I took the risk of using a financial planning model from Personal Capital. I liked it because you could put all your assets into their model, generate multiple scenarios (your retirement age, your children’s college costs, home costs, etc.), and then run Monte Carlo simulations for the years ahead, including whether you have enough money left for retirement. Combining the information from this power team and my own use of the modeling tool, I was able to put together a plan and set a budget for our future potential home.
On Monday, the day after the open house, I started drawing up a list of “must-haves” and “nice-to-haves” for a future three-bedroom apartment. I was surprised to find that the superstar broker responded quickly to my email, suggesting a meeting on Tuesday night at our home. She explained that she really likes to get to know her clients’ true needs, and that being in our home provides important insights into how we really live and what our true priorities are. Because things were moving so fast, I didn’t even have a chance to review my list of “must-haves” and “nice-to-haves” with Amy before we met with the real estate broker. Luckily, she thought I had made a good list.
Our realtor was as amazing as advertised. She arrived with three bound volumes: the first was a book of various three-bedroom apartments for sale in our neighborhood, complete with pictures and floor plans; the second was a book of the sales of all the two-bedroom apartments in the ~25-year history of our building; and the third was a book explaining how best to arrange one’s apartment visually for showing. In turn, the realtor was impressed by my list of about eight “must-haves” and a similar number of “nice-to-haves.” After spending about an hour together, she promised to get back in touch with a proposed plan of action.
A week later, we spent a day seeing apartments together. We managed to see about 15 in 6 hours, including the lunch break. That day was a whirlwind, and while we ended with some vague possibilities, none really struck us. Our realtor suggested several open houses to visit on the weekend without her. We dutifully went, and voilà! We saw the winner that Sunday. A beautiful three-bedroom 2,000-square-foot apartment, a relative palace. It had a large California-style kitchen, rare in Manhattan, that I prefer for entertaining (we cook for friends a lot). The two additional bedrooms were the same size, which was perfect for our twin girls.
About 19 days after I went to that first open house with Alice, we had an accepted offer on the apartment, possibly a speed record for our broker. She commented that she and her associate discussed hanging a picture of me as their favorite client in their careers. Of course, this could just be part of her salesmanship to make me feel good, but she seemed earnest. She commented that the most challenging part of her job is how uncertain most people are in their thinking, in contrast to the clear priorities with which I pursued everything.
Amy doesn’t operate as decisively, so initially, she was hanging on for dear life. It was a lot to take in. How much house could we afford, how long could we manage two mortgages while we hadn’t sold our home, how much risk were we taking on, and does she truly love the new apartment? In the context of our long marriage, she has come to trust my judgment about big decisions, although ones of this magnitude are understandably challenging. Luckily, we are now eight years out from that decision, and I think both Amy and I feel it was a good one.
The buying of our new three-bedroom home was exactly the project I needed to recover from my depression and inability to act. That first day when I started emailing friends to get their contacts, such as the superstar real estate broker, it unlocked my inability to connect with my friends. I was finally reaching out—the need for professional assistance was enough to motivate me to take action. I recognized this activation and used it to reach out to friends who had nothing to do with buying a home.
When you are depressed, it is an extremely lonely place. No one understands what you are going through, not your friends, not your family, not your partner. Amy was wonderfully supportive, but she could do nothing that really helped. Meanwhile, you go through a round-robin of internal dialogue in your mind and think,
“I should reach out to Steve.”
“Well, then again, he hasn’t reached out to me.”
“Ah, I should still reach out to him, but maybe I’ll do it tomorrow.”
That tomorrow leads to another tomorrow, and soon, two-and-a-half years have gone by. I remember using the new energy I had generated from my new home project to finally reach out. Steve was delighted to hear from me and asked why there was a long gap. When I explained it to him, I was shocked to discover that he also suffered from chronic depression, so he immediately understood. The other thing I found out was his relief that it wasn’t simply that he had lost me as a friend. It turned out that he had a trauma that dated all the way to being a 13-year-old adolescent, when he was best friends with two other boys until, suddenly, one day he was out and the two others kept being best friends. No explanation. That abandonment continued to be a paralyzing source of fear for him. I apologized profusely, and we made a date to get together for dinner later that week, where we had a joyous reconnection.
It was so fascinating to me to realize that on the other side of my depression, friends like Steve were themselves struggling with their own troubles and interpreting my absence from a completely different perspective. One of the things I gained from my experience with depression was a newfound empathy for the entirety of human existence. While I believe I was sympathetic to my patients, who often suffered from mental illness and whom I prescribed remedies like antidepressants or antianxiety pills, my ability to put myself in others’ shoes had shifted entirely. While I wouldn’t wish the horrible trial of going through major depression, I now consider it a gift.
By the end of that week, when I started looking for a new apartment, I was basically myself in terms of my mood. The wonder and joy of being alive had come back. It almost seemed strange to imagine once again being numb to all happiness. Medically speaking my recovery is quite unusual. Eventually, I needed a letter from my psychiatrist stating that I had indeed recovered from my depression for an application for a life insurance policy. When I told him what had happened and how I had finally recovered from my depression, he said he had never had another patient with a similar experience. He sheepishly asked to speak to Amy to confirm the details.
Now that I have recovered, one thing many friends ask me is whether I am worried that I may suffer from another episode. Most patients who have had a major depressive episode do have another, or several additional episodes. However, there is a wide range of outcomes. In my case, I feel confident that this won’t happen again, but if it does, I’ll just buy another home (just kidding)!
Brilliantly vulnerable and relatable. Good piece, Chris.